High Altitude Illness: The Essentials
Author: Dr. George Rodway

Author: Dr. George Rodway
Prevention of high-altitude illness is greatly preferred to treatment of high altitude illness. In other words, judgment, not medications, is of primary import when travelling to high altitude.
Sojourners are traveling to the mountains of Asia, North America, Europe, and South America in ever increasing numbers for a variety of recreational, business, and lifestyle-oriented reasons. Skiing, hiking, mountain climbing, and other tourist activities are commonly undertaken in these geographic regions by individuals who normally reside at or near sea level. Unfortunately, a significant percentage of persons who travel to elevations over 2500 m develop signs and symptoms of high-altitude illness. At higher altitudes, the risk may increase.
High altitude illness, in the form of high altitude pulmonary edema (HAPE) or high altitude cerebral edema (HACE), is potentially fatal. Both conditions, in addition to a less serious, but more common form of high altitude illness, acute mountain sickness (AMS), typically develop in unacclimatized persons shortly after ascent to high altitude.
Several factors, including the rate of ascent to altitude, final altitude reached, altitude at which an individual sleeps, and individual physiology are believed to influence development of these conditions. Additional risk factors include pre-existing chronic heart and lung conditions, residence at low altitude, prior history of high altitude illness, and level of exertion at altitude.
Atmospheric pressure and the partial pressure of oxygen decrease rapidly at increasing altitude. The partial pressure of oxygen is also lowered as one moves toward the poles of the earth at any given altitude. The large cold air mass in the stratosphere above the equator (but not the poles) compresses the air mass below it, creating a denser atmosphere in the equatorial and temperate regions. The barometric pressure on the summit of Mt Everest, 8848 m in elevation, is approximately 253 mmHg at latitude 27 degrees north. If Mt Everest were at the same latitude as Mt McKinley (Denali) in Alaska, USA, 6194 m elevation and 62 degrees north, the estimated barometric pressure would be 222 mmHg. This considerable barometric pressure difference would likely make Everest, if located at a latitude similar to McKinley, a nearly insurmountable physiological challenge without supplemental oxygen. It should also be noted that barometric pressure is known to fluctuate with changing weather systems and the seasons.
During ascent to high altitude, the blood becomes hypoxemic causing a series of physiological responses. This process is called acclimatization and helps adapt the human body to the hypoxic environment. Hypoxemia (low blood oxygen) causes hyperventilation, resulting in an increase in arterial blood oxygenation.
Acute mountain sickness (AMS) is a common affliction in otherwise healthy individuals who go rapidly to high altitude. Spanish missionaries are credited with some of the earliest descriptions of the malady in writings about their experiences in the high altitude areas of South America in the 16th and 17th centuries. In 1913, Thomas Ravenhill, a medical officer employed by a Chilean mining company located approximately 4500 m above sea level, provided the first modern account of AMS. The mines were served by a quick ascending railway, so he had the opportunity to observe miners suffering the effects of high-altitude, uncomplicated by the fatigue, cold, or lack of food that confounded previous descriptions by explorers and mountain climbers.
AMS is defined as the presence of a combination of nonspecific symptoms that appear within a few hours after ascent to altitude, e.g., headache, loss of appetite, nausea, vomiting, weakness, lassitude, dizziness, and difficulty sleeping. The symptoms of mild to moderate AMS are typically maximal on day two or three after rapid ascent, and often disappear by day five. On further ascent to higher altitude, symptoms may reappear. AMS is usually a benign, self-limited condition in its mild and moderate forms. Severe AMS can quickly progress to HACE, a form of high altitude illness that is potentially lethal and which will be discussed subsequently in greater detail. By definition, abnormal neurological signs or symptoms are not part of an AMS diagnosis. Neurological
dysfunction (eg, ataxia or altered consciousness) indicates the transition to a life-threatening form of altitude illness.
The incidence of AMS depends upon the rate of ascent and the ultimate altitude reached by the individual. However, the ascent rates that will predispose or prevent AMS are not known with certainty.
Gradual ascent that allows for acclimatization is universally accepted as the best strategy for the prevention of high altitude illness. Day trips to higher altitude involving mild to moderate exercise, with a return to lower altitude for sleep, aid acclimatization. Conversely, over-exertion early in altitude exposure contributes to altitude illness. Physiological stressors (e.g., hard exercise and cold) may play a significant role in high altitude morbidity. A number of published guidelines regarding ascent rate and the use of rest days during ascent to high altitude are available, and all make similar recommendations. These can be conservatively summarized as follows: Above 3000 m, limit daily sleeping altitude ascent to 300 m/day, with a ‘rest day’ every 2-3 days during which the climber sleeps at the same altitude on the second night. The Table proposes risk categories of altitude illness for those exceeding suggested ascent rates and/or having a history of severe altitude illness.
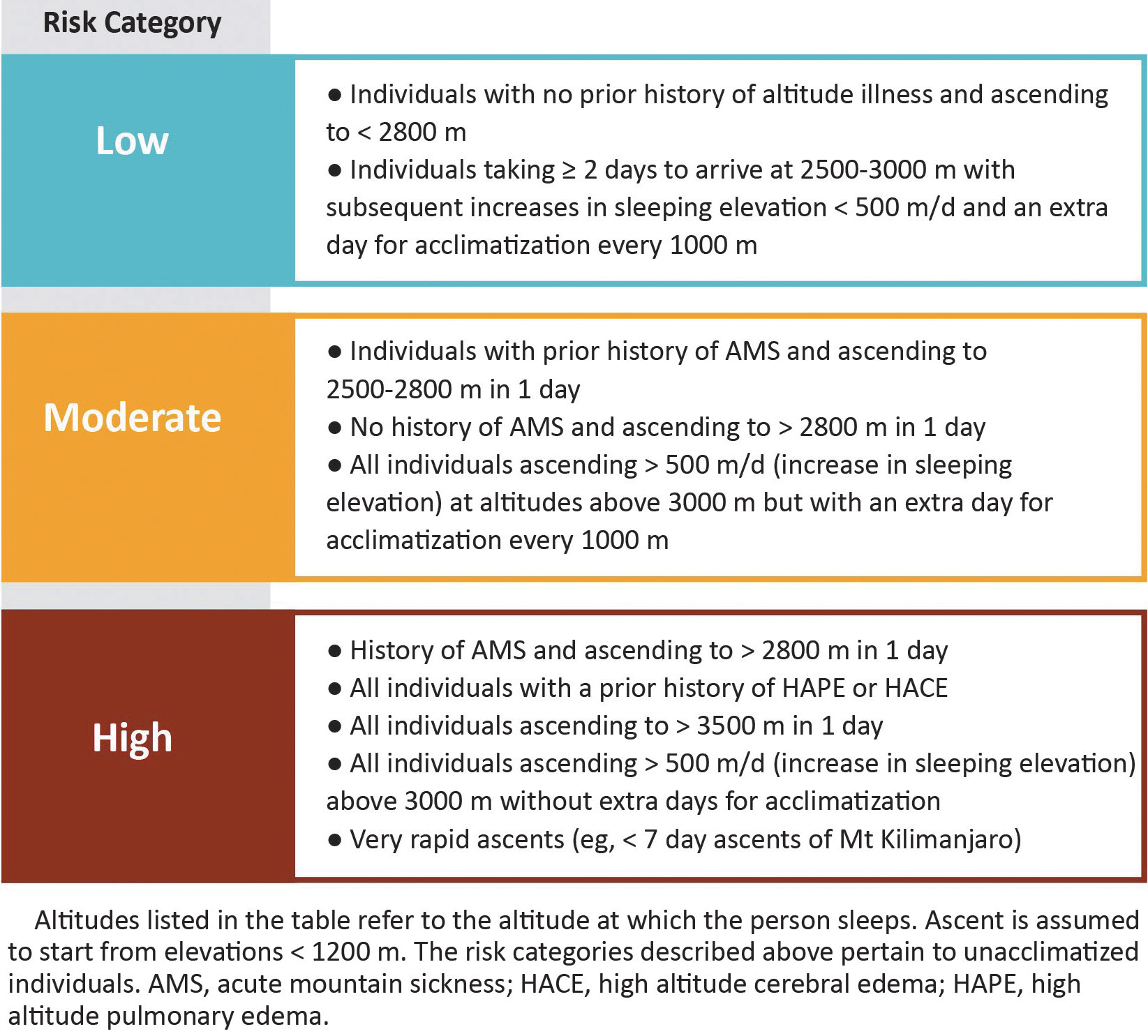
Those in the moderate or high-risk categories may choose to be more conservative in their ascent profiles and include more rest days than typically recommended.
AMS is commonly misdiagnosed as a viral flu-like illness, hangover, dehydration, exhaustion, or a medication effect. Uncomplicated AMS is not associated with flulike symptoms of fever or myalgia. Response to fluids will help differentiate dehydration (symptoms of weakness, headache, and nausea) from AMS, as fluid administration alone will not improve AMS. However, exhaustion may also cause weakness, lassitude, headache, and irritability, thus making it difficult to distinguish from AMS.
The severity of initial clinical presentation of AMS is not predictive of ultimate disease severity. Therefore, careful monitoring for symptom progression is essential. Mild AMS can often be effectively treated by remaining at the same elevation and waiting one to three days for the body to acclimatize. Exertion should be minimized during this period, but occasional light exercise can be encouraged as it increases blood oxygen saturation. If available, low flow supplemental oxygen can provide remarkable relief, especially at night. During sleep, blood oxygen saturation levels are likely to drop, increasing the possibility of an exacerbation of AMS symptoms.
Three important axioms should guide decisions: (1) persons with suspected altitude illness should not ascend higher; (2) no improvement or worsening of conditions should prompt descent to lower altitude; and (3) neurologic changes (ataxia or altered consciousness) should prompt immediate descent to a lower altitude. In many cases, a modest descent (500 to 1000 m) will resolve symptoms of mild to moderate AMS. Severe AMS symptoms require a further descent and possibly medical management.
Simulated descent with a portable hyperbaric [high pressure] chamber (eg, Gamow bag) has proved to be effective in resolving the symptoms of mountain sickness. Typically
used in cases of moderate to severe altitude sickness (eg, HACE or HAPE), these fabric devices allow the patient to be rapidly taken to a simulated altitude that is approximately 2000 m lower.
When descent is not possible or practical (and assuming a hyperbaric chamber or supplemental oxygen are not readily available), pharmacological therapy becomes necessary. Unless a patient has known elevated liver function test values or is allergic to sulfa drugs, the standard therapy is acetazolamide. Acetazolamide is also used to treat high altitude insomnia brought on by nocturnal periodic breathing. This medication is believed to promote sleep via improved nocturnal oxygenation and subsequent decrease or resolution in the periodic breathing pattern. Sedating sleep-inducing agents should be avoided because of the risk of respiratory depression and an associated drop in blood oxygen saturation.
Dexamethasone is another effective treatment for all degrees of AMS. No data exists to suggest whether the combination of acetazolamide and dexamethasone, with their different mechanisms of action, is superior to the use of either agent alone. Although conclusive evidence to support the practice is lacking, some argue to use dexamethasone to relieve symptoms and acetazolamide to speed acclimatization. Some also believe that those who require dexamethasone should descend, as this powerful medication may produce a euphoria that could mask the progression of AMS symptoms. Furthermore, the potential adverse effects of dexamethasone are numerous, and as such should be administered for a period of less than one week.
Relief from specific symptoms of AMS can be obtained with other medications. Ibuprofen in a single dose can ameliorate high altitude headache, and antiemetics can be used to treat the nausea and vomiting that can accompany AMS.
High altitude cerebral edema (HACE) is a clinical diagnosis, defined as the onset of ataxia, altered consciousness (including confusion, impaired mentation, drowsiness, stupor, and coma), and severe lassitude. Headache, nausea, and vomiting are frequently present.
HACE may develop as a progression of AMS, or may emerge without preceding AMS symptoms. Deterioration from HACE to coma may be rapid. The progression may be as fast as 12 hours, but usually requires one to three days. In one recorded case, coma occurred within 24 hours and death within 48 hours after high altitude exposure. Not surprisingly, severe HACE and HAPE may occur in the same individual. When HACE predominates in fatal cases of high altitude illness, autopsy findings reveal brain herniation as the cause of death.
The same general principles of preventing AMS also apply to HACE. Plan a slow and reasonable ascent rate with gradual sleeping altitudes and an appropriate number of rest days. Limit physiological stressors such as heavy exercise.
It has been suggested that the most sensitive indicator for HACE may be ataxia, which is best evaluated via the tandem gait test. This is performed by asking the subject to walk in a straight line by touching the heel of the forward foot to the toe of the other foot
with each step. Failure to perform these coordinated movements makes it more likely that the patient is suffering from HACE.
Early recognition of HACE is essential for successful treatment. Severe AMS or a rapid progression from mild to moderate, or from moderate to severe AMS, should prompt aggressive management. Descent should ideally be started in cases of suspected severe AMS, or at the very latest, at the first sign of ataxia or change in consciousness. Descent of at least 500 to 1000 m (or hyperbaric therapy) and supplemental oxygen are ideal treatments when practical and/or available, either singly or in combination. For severe illness, the combination provides optimal therapy. In addition, dexamethasone can be administered, and, if available, oxygen applied and titrated to keep blood oxygen saturation above 90%.
Empiric evidence suggests HACE responds well to descent, dexamethasone, and oxygen if given early in the course of the illness. Sequelae from HACE can last weeks, but full recovery is common. Outcomes are less promising if descent, dexamethasone, and oxygen are initiated after the patient is unconscious. Coma may persist for days, even after evacuation to low altitude, or can progress to death.
One of the earliest and best-described references to high altitude pulmonary edema (HAPE) occurred with the 1894 (1898 English) publication of prominent Italian physiologist Angelo Mosso’s seminal volume, Life of Man in the High Alps. He describes a young soldier who ascended to a hut on the summit of Monte Rosa (4634 m), developed a severe headache, cyanosis, shortness of breath, very rapid heartbeat, and pink frothy sputum, but no fever or chills. He was thought to have pneumonia and recovered after several days at the summit hut without treatment—a most fortunate young man. In retrospect, this account is a perfect description of HAPE. The misconception that HAPE was pneumonia persisted for decades, and it was not universally recognized as a unique entity until 1960. Today, HAPE accounts for the majority of deaths from high-altitude illness.
As with AMS and HACE, the incidence of HAPE is related to the rate of ascent, the altitude reached, and individual susceptibility. Additional nervous system stimulation from exertion and cold will also contribute to an increased risk for developing HAPE. Upper respiratory tract infection or bronchitis may be precipitating factors, as well.
Special precautions are necessary during ascent to altitude in individuals who have previously experienced HAPE. After an episode of HAPE, future ascents to high altitudes should be conducted more slowly, and with particular vigilance for early symptoms of high altitude illness. As in the case of AMS/HACE prevention, the same principles of ascent rate, rest days, sleeping altitude, and physiological stressors apply.
The initial onset of HAPE is usually at night or early morning, one to three days after ascent is initiated. In the setting of a recent altitude gain, at least two of the following symptoms must be present in order to qualify as a diagnosis of HAPE: shortness of
breath at rest, cough, weakness or decreased exercise performance, chest tightness, or congestion. In addition, at least two of the following signs must be present: crackles or wheezing in at least one lung field, cyanosis, or rapid heart-beat at rest. Severe hypoxemia is often apparent when measured with pulse oximetry.
Cerebral signs and symptoms commonly accompany those of HAPE. Approximately 50% of those with HAPE have AMS, and 14% have HACE. Of those HAPE victims whose condition deteriorates and fatality results, 50% have HACE at autopsy.
Oxygen and descent are the mainstays of HAPE treatment. Supplemental oxygen (as well as descent) increases the blood oxygen saturation and benefits the brain by improving neuropsychological status, especially higher functions such as memory and affective behaviour such as mood. Mild and some moderate cases of HAPE can be treated with rest at the same altitude (i.e., without descent) and supplemental oxygen for 48 to 72 hours. If the patient does not improve, descent is recommended. Moderate or severe HAPE should prompt an immediate descent of at least 500 to 1000 m, or until the symptoms resolve. The patient should be carried or evacuated by another means (e.g., helicopter) that does not require exertion. Descent, supplemental oxygen, or both are nearly always successful. Repeat ascent should not be attempted until full recovery, and only then with caution. As with severe AMS or HACE, hyperbaric therapy is also useful.
Monitoring blood oxygen saturation by pulse oximetry is recommended to guide therapy. Patients with severe HAPE (blood oxygen saturation < 90% five minutes after initiating high flow oxygen), as well as those with concomitant HACE, must be moved to a lower altitude and possibly hospitalized. Medication (nifedipine) becomes necessary if supplemental oxygen is unavailable or descent is impossible.
Prevention of high-altitude illness is greatly preferred to treatment of high altitude illness. In other words, judgment, not medications, is of primary import when travelling to high altitude. The high altitude sojourner must know when to descend to lower elevations in order to avoid high altitude illness, or to lessen its severity. As such, basic rules can be very helpful in this environment: if one is ill at altitude, assume that the symptoms are due to altitude until proven otherwise; if one has altitude symptoms, do not ascend; if one is quite ill and/or is getting worse (or cannot walk heel-to-toe in a straight line), descend immediately. Finally, anyone with altitude illness should be observed or accompanied (if descending) by a responsible and competent companion.
George W. Rodway, PhD, represents a combination of scientific researcher, mountaineer and science writer. An Associate Clinical Professor at the University of California, Davis (USA), his academic work focuses on the cardiopulmonary response to hypoxia and it has on occasion presented him with the opportunity to climb mountains with scientific intent. An active mountaineer since the late 1970s, he has climbed in Canada, Mexico, Europe, the US, and the Himalaya. He serves international organizations such as the International Society for Mountain Medicine and the Medical Commission of the Union Internationale des Associations d’Alpinisme (UIAA).